Wrong site surgeries
How Common Are Wrong-Site Surgeries? A Breakdown by Medical Specialty
Wrong-site surgery — operating on the wrong body part, wrong level, wrong procedure, or even the wrong patient — is classified as a “never event” in modern healthcare. These incidents are rare, but they still occur despite extensive safety protocols.
Across all surgical fields, estimates suggest wrong-site surgeries happen in roughly 1 out of every 50,000 to 100,000 procedures. However, risk is not evenly distributed. Some specialties see higher rates due to the nature of anatomy, workflow complexity, or case volume.
Below is a specialty-by-specialty breakdown of where these events most often occur and why.
Orthopedics: The Highest Share of Cases
Orthopedic surgery accounts for the largest proportion of reported wrong-site events.
Common scenarios:
Operating on the wrong limb (left vs. right knee or shoulder)
Wrong finger or toe
Incorrect implant or procedure type
Why risk is higher:
The body has paired structures (arms, legs, hands, feet)
Many procedures involve small anatomical targets like digits
High daily case volume with similar operations scheduled back-to-back
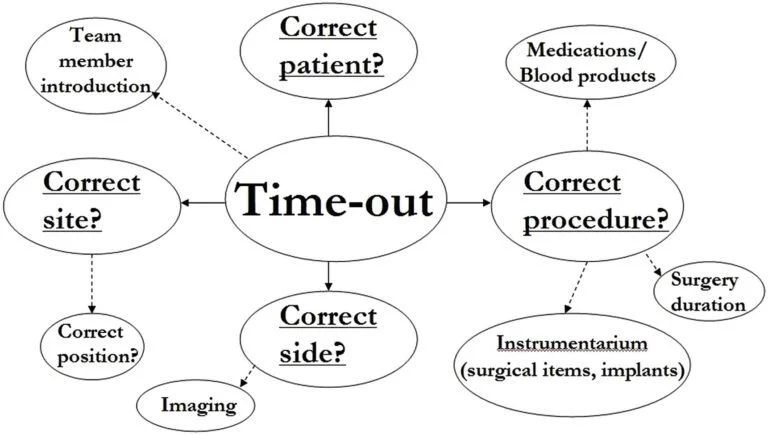
Key safety practices:
Clear site marking with initials and directional arrows
Team confirmation of side and procedure during a surgical “time-out”
Imaging displayed and verified before incision
Neurosurgery and Spine Surgery: Level Identification Challenges
Spine procedures represent the second most common category for wrong-site events.
Common scenarios:
Operating at the wrong vertebral level (for example, L4–L5 instead of L5–S1)
Wrong side during cranial or nerve procedures
Why risk is higher:
Vertebrae look very similar from level to level
Prior surgeries can alter normal anatomy
Errors can occur when counting levels on imaging
Key safety practices:
Intraoperative imaging to confirm the exact level
Multiple team members verifying anatomy before proceeding
Formal localization before incision
General Surgery: Verification and Documentation Risks
General surgery has a moderate share of wrong-site events, often tied to communication or documentation breakdowns.
Common scenarios:
Wrong side for hernia, breast, lung, or kidney procedures
Wrong procedure due to scheduling or consent mismatch
Wrong patient in rare cases involving chart errors
Why risk occurs:
Multiple similar procedures scheduled on the same day
Last-minute changes to operative plans
Incomplete or inconsistent documentation
Key safety practices:
Cross-checking consent forms, schedules, and imaging
Team briefings that confirm diagnosis and surgical plan
Hard stops if any discrepancy is found
Ophthalmology: High Volume, Small Margin for Error
Although the total number of incidents is lower, ophthalmology has a notable rate relative to its extremely high procedural volume.
Common scenarios:
Surgery on the wrong eye
Implanting the wrong intraocular lens during cataract surgery
Why risk occurs:
High throughput environments
Short procedures performed consecutively
Confusion caused by laterality abbreviations (OD/OS)
Key safety practices:
Prominent marking above the correct eye
Verbal confirmation of lens type and power before implantation
Strict adherence to time-out protocols
ENT, Urology, and Other Specialties: Lower Overall Rates
These fields see fewer wrong-site events overall but still face specific risks.
Common scenarios:
Operating on the wrong sinus or ear
Wrong side for kidney or testicular procedures
Removing the wrong lesion when multiple are present
Why risk occurs:
Bilateral anatomy
Multiple possible surgical targets
Ambiguous diagrams or abbreviations
Key safety practices:
Precise marking of the exact lesion
Imaging confirmation when appropriate
Clear labeling and documentation
Why These Errors Still Happen
Even with strict protocols, wrong-site surgeries usually stem from system failures rather than individual mistakes. The most common contributing factors include:
Communication breakdowns during handoffs
Skipped or rushed safety checklists
Inadequate site marking
Documentation inconsistencies
Fatigue and workflow pressure
How Hospitals Reduce Risk
Most surgical facilities use a standardized three-step safety process:
Pre-procedure verification – confirming patient identity, procedure, and site
Site marking – performed by the surgeon before the patient enters the operating room
Time-out – a final team-wide pause immediately before incision
These steps have significantly reduced the rate of wrong-site surgeries over time.
What Patients Can Do to Add a Safety Layer
Patients can play a small but meaningful role in prevention:
Clearly state the procedure and side to each provider involved
Confirm that the surgeon marks the surgical site while you are awake
Ask whether a time-out will be performed before the procedure begins
These simple actions reinforce the safety system already in place.
Final Perspective
Wrong-site surgeries are rare events, but they remain a serious patient safety concern. Orthopedics and spine surgery account for the largest share, largely due to paired anatomy and complex localization. Other specialties experience lower rates but face their own unique risks.
The good news is that modern safety protocols — especially checklists, site marking, and team verification — have made these errors far less common than in the past. Continued vigilance from both medical teams and patients remains key to keeping them rare.